|
#1
June 18th, 2016, 01:38 PM
| |||
| |||
| Mds hc
Hello sir I am here as I want to get the Minimum Data Set - Home Care (MDS-HC) form so will you please provide me the form?? Hey as you said that you want to get the Minimum Data Set - Home Care (MDS-HC) form so here I am providing you that: Minimum Data Set - Home Care (MDS-HC) form 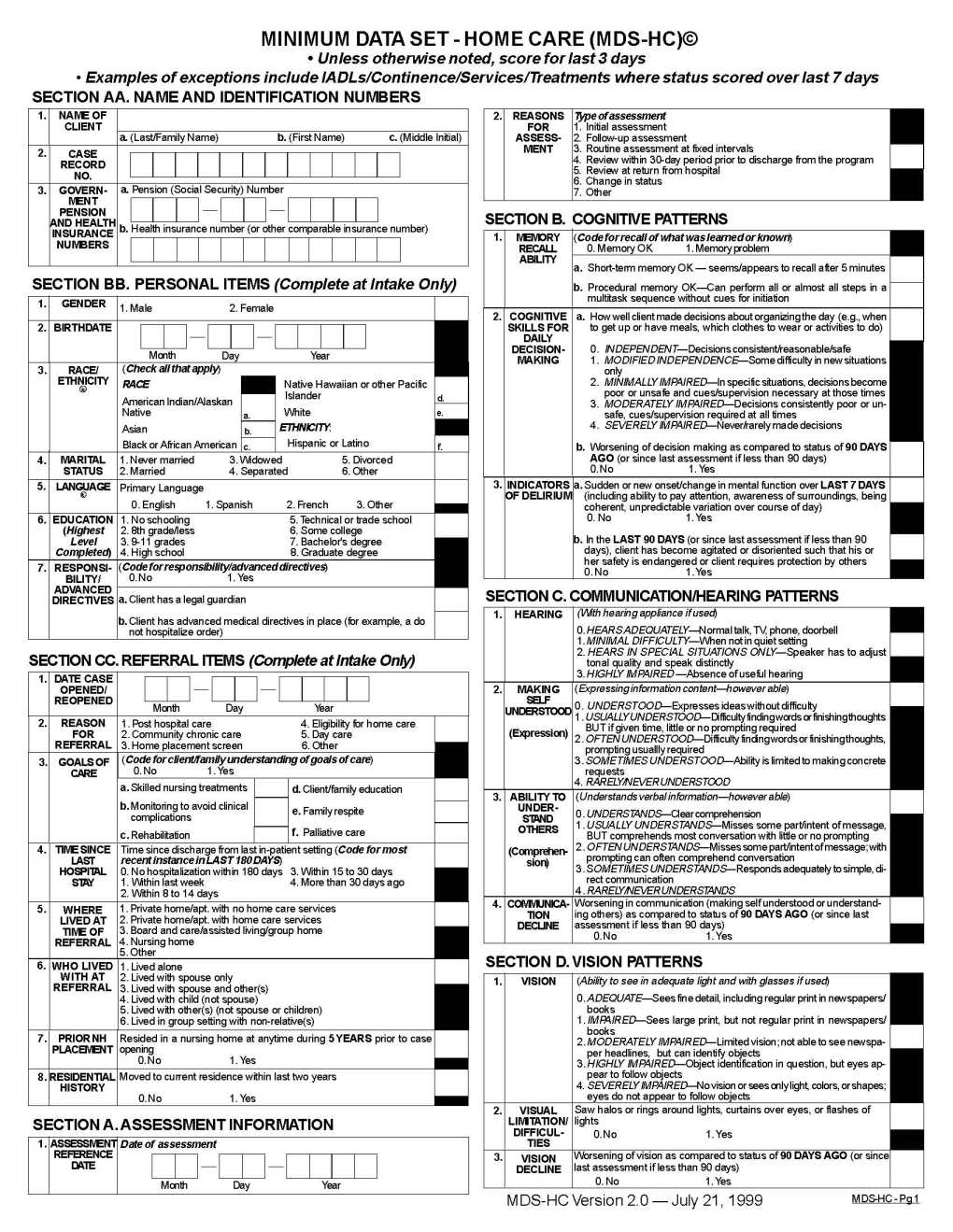    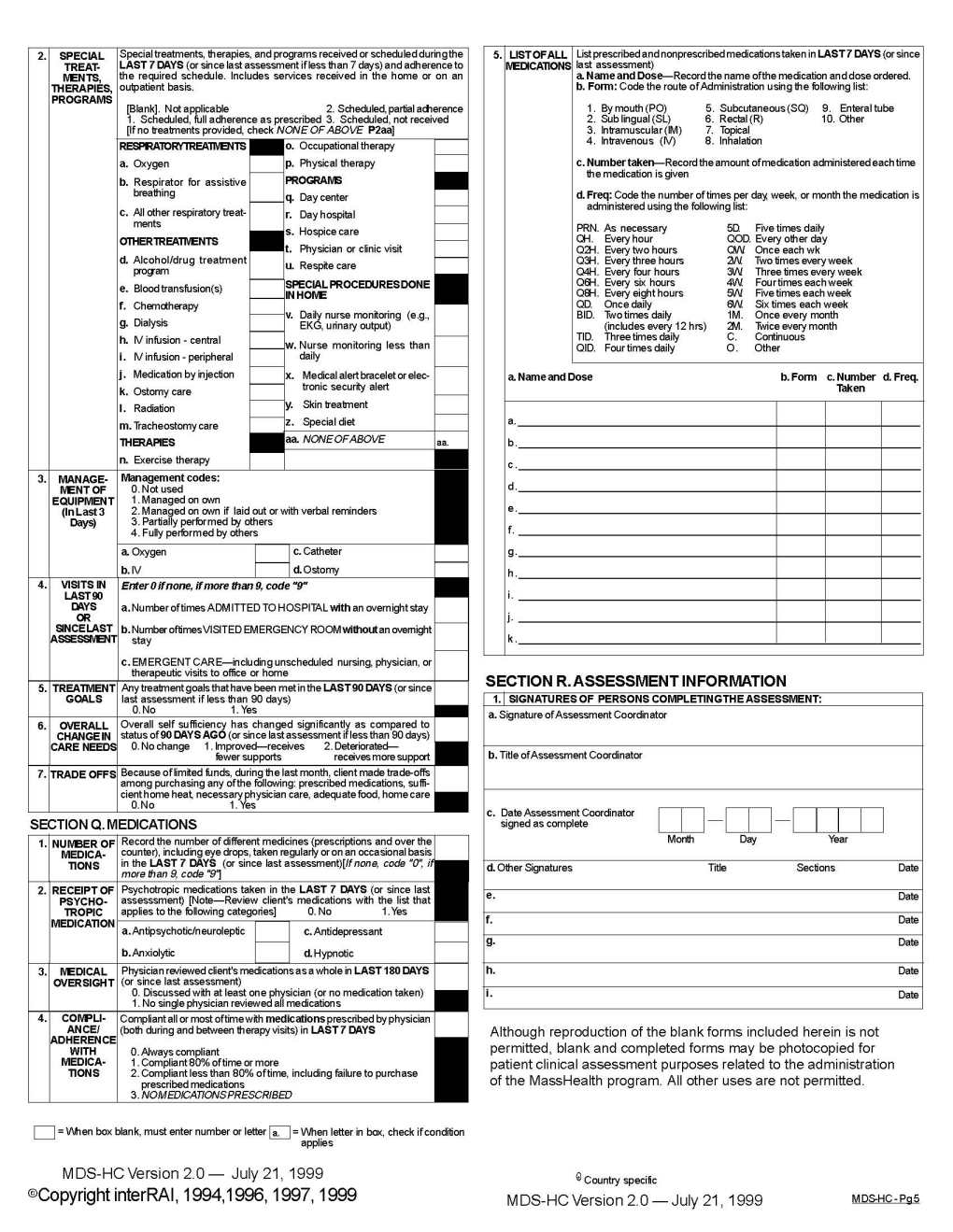 Details to be filled in this form are: SECTION AA. NAME AND IDENTIFICATION NUMBERS 1. NAME OF CLIENT 2. GOVERNMENT PENSION AND HEALTH INSURANCE NUMBERS 3. a. Pension (Social Security) Number b. Health insurance number (or other comparable insurance number) SECTION BB. PERSONAL ITEMS 1. Male 2. Female 2. BIRTH DATE 1. GENDER 2. REASONS FOR ASSESSMENT Type of assessment 1. Initial assessment 2. Follow-up assessment 3. Routine assessment at fixed intervals 4. Review within 30-day period prior to discharge from the program 5. Review at return from hospital 6. Change in status 7. Other Saw halos or rings around lights, curtains over eyes, or flashes of lights SECTION B. COGNITIVE PATTERNS 1. MODIFIED INDEPENDENCE 2. MINIMALLY IMPAIRED 3. MODERATELY IMPAIRED 4. SEVERELY IMPAIRED Last edited by Neelurk; March 3rd, 2020 at 08:33 AM. |